Chapter Two — Joint Movement
Observation of movement indicates a complex and seemingly infinite variety of positional changes which are controlled by a variety of internal and external factors.
Internal structures are the type of joint, the planes in which movement can occur at a joint and the muscles and nerves supplying the joint.
The external structures are the lever arm, the centre of mass, the gravity influencing the movement at the joints.
During dynamic contraction or muscle stretching, the muscle involved will change length.
If a muscle contract from its lengthened position and continues contracting until its short as possible= full range of motion.

Muscle length is skeletal muscle in your body, when at resting length, is at its optimal length for development of force, testing involves elongating the muscle in the direction opposite of its action while assessing its resistance to passive lengthening. In other words, muscle length testing assesses the resistance/ease to passive movement. This is in contrast to typical flexibility or ROM testing.
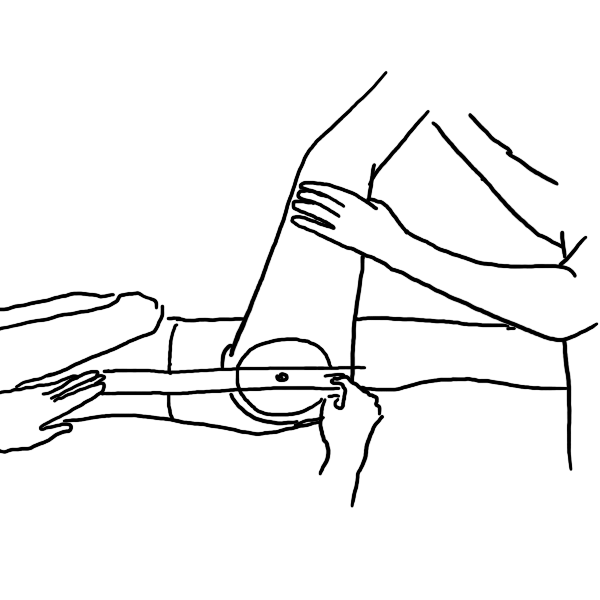
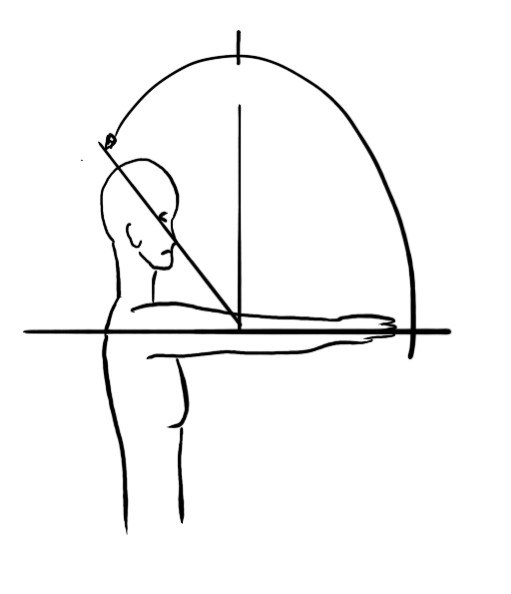
A goniometer is an instrument that measures an angle that a joint moves in active range of motion or passive range of motion.
The term goniometry derives from two Greek words, gōnia, meaning angle, and metron, meaning measure
Active Movement: The patient performs the movement.
Active Assisted Range of Motion (AAROM)
Movement of a joint or limb in which the patient provides some effort, but also receives some assist from an outside force.
Mechanical Assistance: When the assistance is applied by mechanical tools as. slings. Pulleys.
Physiological movement can only achieved actively through the contracting of the patients muscles to produce normal movement.
Accessory movements are movements that can only be achieved by an external force, these movements cannot be achieved through muscle contraction BUT by manipulating the joint to produce this movement.
Balance The ability to align body segments against gravity to maintain or move the body (centre of mass) within the available base of support without falling; the ability to move the body in equilibrium with gravity via interaction of the sensory and motor systems.
Cardiopulmonary fitness The ability to perform low intensity, repetitive, total body movements (walking, jogging, cycling, swimming) over an extended period of time.
CoordinationThe correct timing and sequencing of muscle firing combined with the appropriate intensity of muscular contraction leading to the effective initiation, guiding, and grading of movement. It is the basis of smooth, accurate, efficient movement and occurs at a conscious or automatic level.
Flexibility The ability to move freely, without restriction; used interchangeably with mobility.
Mobility The ability of structures or segments of the body to move or be moved in order to allow the occurrence of range of motion (ROM) for functional activities (functional ROM). Passive mobility is dependent on soft tissue (contractile and noncontractile) extensibility; in addition, active mobility requires neuromuscular activation.
Muscle performance The capacity of muscle to produce tension and do physical work. Muscle performance encompasses strength, power, and muscular endurance.
Neuromuscular controlInteraction of the sensory and motor systems that enables synergists, agonists and antagonists, as well as stabilizers and neutralizers to anticipate.
Stability, and equilibrium: Used interchangeably with static ( balance in a stationary position) or dynamic balance (balance in motion/whilst moving).
Stability The ability of the neuromuscular system through synergistic muscle actions to hold a proximal or distal body segment in a stationary position or to control a stable base during superimposed movement. Joint stability is the maintenance of proper alignment (tendency of structures to be in a straight line) of bony partners of a joint by means of passive and dynamic components.
Agonist or Prime Mover: refer to muscles that play a major role in initiating, carrying out and maintaining a particular movement. E.g. Psoas major in hip flexion.
Antagonist:refers to muscles that act in direction opposite the agonist. E.g. gluteus maximus, hamstring group.
Assistant movers: muscles which perform movement similar to agonist but play a less significant role. E.g. sartorius or rectus femoris in hip flexion.
Stabiliser or Fixator: contract to control the position of the bone so that it act as a base from which the agonist can contract. E.g. trunk muscles stabilising the pelvis during hip flexion.
A synergist: act together or to produce combined action. True synergist vs helping synergist.
An end feel is defined as the sensation or feeling which the therapist detects when the joint is at the end of its available PROM. There are several end feels that are used. ... In a pathological joint with a bony end feel, the sensation will happen before the expected end range of motion.
Is to make stable, steadfast, or firm, to hold steady: such as to maintain the stability of (something, such as an airplane) by means of a stabilizer.
Stabilization training is an active form of physical therapy designed to strengthen muscles to support the spine and help prevent lower back pain. Through a regimen of exercises prescribed by a physical therapist, the patient is trained to find and maintain his/her "neutral spine" position.