Overview of Training Materials: Promoting Equitable Access to Health Care for Households
Prepared by Di McIntyre
Health Economics Unit, University of Cape Town
Background
The idea for developing this set of training materials arose from the ‘Affordability Ladder Program’ (ALPS). The ALPS initiative focused on the experience of households of illness and of seeking health care. As the name would suggest, a key focus of ALPS was that of affordability and other aspects of access to health care for households. The ALPS team recognised that almost all of the training materials presently available focus on illness and health services from the health system’s perspective, with little or no attention devoted to the perspective of households. In addition, few of the available materials focus explicitly on the issue of equity, which should be seen as a priority in the context of growing awareness of substantial inequities in existing health systems; the majority of training materials are presently directed towards efforts to promote efficiency of health services. This was seen as an important gap, in that health care managers and policy makers will be better placed to design and implement health care policies and detailed plans that meet population needs if they are aware of the experience of households and if equity is the ‘lens’ through which alternative policies are considered. Finally, despite access to health care being a key policy objective by many countries, there is a lack of clarity about how access is defined and what constitutes access. It is, thus, also important to explore the different aspects of access in greater detail so that equitable access can become a reality. On this basis, it was decided to develop a set of training materials that present participants with an equity ‘lens’ through which to view the challenges of promoting health system access, focussing attention on households’ experience of illness and health service access.
Key objectives
The key objectives guiding the development of these training materials were that they should provide a basis to:
- Develop an understanding of the dimensions of access to health care;
- Create greater awareness of health care access constraints from the household perspective;
- Promote critical evaluation of policy options to address access constraints in relation to equity goals; and
- Promote and strengthen effective development and implementation of equitable health sector policies.
Target groups
The training materials can be used for a diverse set of target groups, but are primarily aimed at current and future health sector managers. The materials are presented in a format that can be used for a one-week short course for health sector managers. However, the materials are sufficiently flexible to be used in different contexts. In particular, it is envisaged that the case studies can be used on an ad-hoc basis in post-graduate programs such as Masters in Public Health programs. In this case, individual case studies may be used where they meet a need within an existing Masters’ module, or the entire set of materials could form the basis for a new Masters module focussing on equitable access issues.
How to use the material
These materials are made available as ‘public domain’ resources and may be used by any public training organisation on a not-for-profit basis (i.e. the materials may not be used for financial gain).
The material is focused around a series of case studies. Each case study is accompanied by a set of facilitator’s notes to assist trainers in using the case studies. These facilitator’s notes:
- outline the objectives of the case study;
- suggest readings that will assist the facilitator in becoming familiar with the key issues raised by the case study and where relevant to prepare a brief input before or after the case study (these readings can also be provided to course participants to further develop their understanding of the key issues addressed by the case studies);
- indicate the time requirements for the case study; and
- provide an overview of the key issues likely to arise in discussion at the end of the case study.
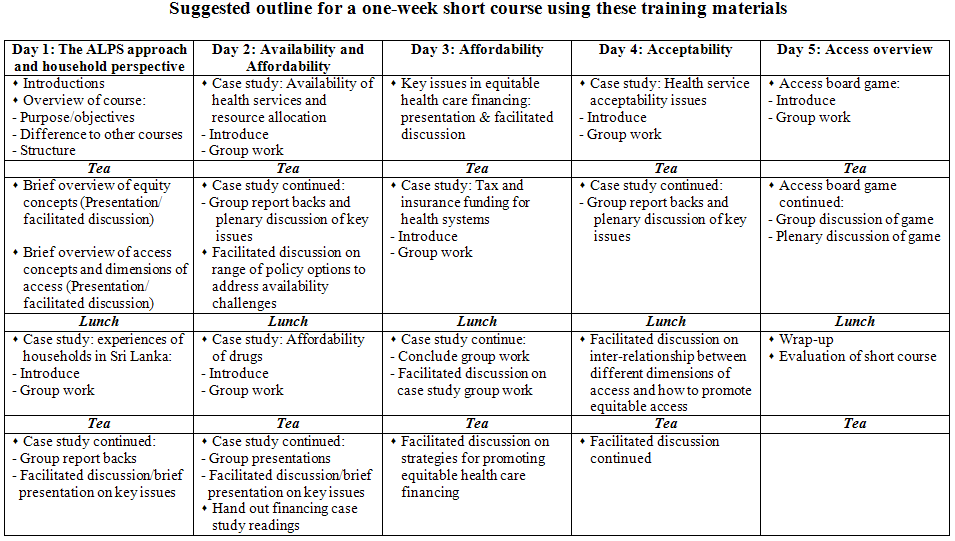
A suggested timetable for a one-week short course using these materials is provided below. Each course convenor should adapt this timetable to suit their preferences (e.g. didactic inputs versus facilitated discussion) and the local context. The basic sequence and flow of materials is structured around the key dimensions of access, which are most commonly identified as:
- Availability, sometimes also referred to as physical access;
- Affordability, sometimes also called economic or financial access; and
- Acceptability, sometimes also called cultural access.
Preparing for facilitating the course
Facilitators using the materials prepared for this course should become familiar with concepts relating to equity in health and health care, access and the household perspective on health services. In addition, health care financing is given particular in the course and it is essential to be familiar with a range of health care financing concepts (including issues such as universal cover, financial protection, risk pooling and financing and benefit incidence). The following list of readings will provide good insights into these concepts and issues.
Equity concepts
- Braveman P, Gruskin S (2003). Defining equity in health. Journal of Epidemiology and Community Health; 57: 254-258. (http://jech.bmj.com/cgi/content/abstract/57/4/254?etoc)
- Braveman P, Gruskin S (2003). Poverty, equity, human rights and health. Bulletin of the World Health Organization; 81: 539-545. (http://www.who.int/bulletin/volumes/81/7/Braveman0703.pdf)
- McIntyre D, Gilson L, Mutyambizi V (2005). Promoting equitable health care financing in the African context: Current challenges and future prospects. Harare: Regional Network for Equity in Health in Southern Africa. (http://www.equinetafrica.org/bibl/docs/DIS27fin.pdf) (especially section 2 and Appendix A)
- Wagstaff, A. (2000). Measuring equity in health care financing: Reflections on and alternatives to the World Health Organization's Fairness of Financing Index. Washington D.C., Development Research Group and Human Development Network, World Bank. (Available on www.worldbank.org).
Access
- McIntyre D, Thiede M, Birch S (2009). Access as a policy-relevant concept in low- and middle-income countries. Health Economics, Policy and Law 4: 179-193.
- Gilson L (2007). Acceptability, trust and equity. In: McIntyre D and Mooney G (eds). The Economics of Health Equity. Cambridge: Cambridge University Press.
Household perspective
- Whitehead, M., Dahlgren, G., & Evans, T. (2001). Equity and health sector reforms: Can low-income countries escape the medical poverty trap? Lancet; 358: 833-836.
- McIntyre D, Thiede M, Dahlgren G, Whitehead M (2005). What are the economic consequences for households of illness and of paying for health care in low- and middle-income country contexts? Social Science and Medicine; 62: 858-865.
- Russell, S. (2004) The economic burden of illness for households in developing countries: A review of studies focusing on malaria, tuberculosis and Human Immunodeficiency Virus/Aquired Immunodeficiency Syndrome. American Journal of Tropical Medicine and Hygiene; 7: 147-155
- Whitehead, M, Dahlgren G, McIntyre D. Putting equity center-stage: challenging evidence-free reforms. International Journal of Health Services; 37(2): 353-361.
- Dahlgren G, Whitehead M (2007). A framework for assessing health systems from the public’s perspective: the ALPS approach. International Journal of Health Services; 37(2): 363-378.
- McIntyre D, Whitehead M, Gilson L, Dahlgren G, Tang S (2007). Equity impacts of neoliberal reforms: what should the policy responses be? International Journal of Health Services; 37(4).
Health care financing
- Kutzin J (2001) A descriptive framework for country-level analysis of health care financing arrangements. Health Policy; 56: 171-204.
- McIntyre D (2007). Learning from experience: health care financing in low- and middle-income countries. Geneva: Global Forum for Health Research. (Available on www.globalforumhealth.org)
- Carrin, G. and James, C. (2004). Reaching universal coverage via social health insurance: key design features in the transition period. Discussion Paper Number 2 - 2004. Geneva: World Health Organization. (Available on www.who.int)
- Gottret, P. and Scheiber, G. (2006). Health financing revisited: A practitioner's guide. Washington, DC: The World Bank. (Available on www.worldbank.org)
Overview of case study materials
Six case studies have been prepared for this course, namely:
- Experiences of households in Sri Lanka: This profiles the personal experiences of illness and health care seeking of four households in Sri Lanka, two of which have someone suffering from diabetes and two with someone suffering from cancer. These households have different socio-economic profiles, which influences their illness and treatment seeking experiences. It serves to focus the attention of participants on the household perspective in relation to health services.
- Availability of health services and resource allocation: This case study considers the availability of health services within a district, relative to the population intended to be served. It highlights that availability of, or physical access to, health services is not simply about the geographic distance to health facilities. It also illustrates how resource allocation strategies can be used to alleviate availability constraints.
- Affordability of drugs in the context of the World Trade Organisation (WTO): The case of India: A key constraint to accessing health care is whether or not households can afford pharmaceuticals. Through means of a role-play, this case study develops an understanding of the WTO’s Agreement on Trade-Related aspects of Intellectual Property (TRIPS) and explores strategies to ensure the affordability of drugs.
- Tax and insurance funding for health systems: Equitable health care financing is critical for promoting health service affordability. An overview of health care financing and related issues in six low- and middle-income countries, two from Africa (Ghana and South Africa), two from Asia (Korea and Sri Lanka) and two from Latin America (Chile and Costa Rica) are presented in this case study. This case study provides an opportunity for analysing factors that facilitate and obstruct equitable health care financing, as well as for developing skills in using a framework that is useful for analysing existing and potential future health care financing mechanisms in country specific contexts.
- Health service acceptability issues: Acceptability is the most neglected dimension of access, but is critical to ensuring equitable access to health care. This case study, presented as a series of media reports, allows participants to develop an understanding of the range of factors contributing to health service acceptability and to explore ways in which health service acceptability can be promoted.
- Access board game: The final case study is a board game which illustrates the full range of health service access constraints that face households. It provides a useful concluding point which draws together the different dimensions of access and which once again focuses participants’ attention on the household perspective.
