Affordability of Drugs in the Context of the WTO - The Case of India: Facilitator Notes
OBJECTIVES OF CASE STUDY
- To develop a critical understanding of the TRIPS Agreement;
- To develop an awareness of the power relations in patent protection;
- To consider the potential impact of the TRIPS Agreement on households; and
- To explore strategies to ensure the affordability of drugs in the context of the TRIPS Agreement.
TIMING OF THE CASE STUDY
This case study will require about 2˝ hours, allocated roughly as follows:
- The first half hour should be devoted to briefly reviewing the background information contained in the case study. This can be done either by the facilitator making a brief presentation or by allowing participants time to read the background information and briefly discussing any questions of clarification. During this time, the facilitator should also divide the group into four groups and assign them stakeholder roles. Each group should be handed their sheet with additional information – these sheets are contained at the end of these facilitator’s notes (they should not be provided with the information made available to other groups).
- The next hour should be reserved for each group to discuss the position they will adopt in their presentation to the Indian Parliament. The facilitator should move between the different groups and particularly encourage participants to ‘adopt the role’ of the group they are representing. The facilitator should also ensure that each group is discussing strategies for ensuring the affordability of drugs.
- Each group will then be allowed a maximum of 10 minutes to present their case (taking a total of 40 minutes).
- The final 20 minutes should be devoted to a brief presentation by the facilitator where the decision of the Indian Parliament on the Patent Act is revealed and where ideas on strategies for ensuring the affordability of medicines are summarised (drawing on the stakeholder presentations and other ideas the facilitator may have).
KEY ISSUES FOR FINAL PRESENTATION
The final amendments to the Patents Act included the following:
- In order to ensure compliance with the TRIPS Agreement, the Patent Act now provides patent protection for both the manufacturing process and final product in the case of new drugs for a period of 20 years.
- However, the amendments explicitly exclude the practice of ‘ever-greening’.
- The amendments also allow pre-grant opposition, whereby any member of the public can oppose the granting of a patent once an application has been publicly announced. This does not ensure that the patent will not be granted, but it does allow public opposition to the issuing of a patent to be mobilised which may influence the patent decision.
- The amendments also explicitly allowed for exporting drugs produced under a compulsory licence to any country (i.e. even if the importing country has not issued a compulsory licence).
- Another critical aspect of the amendments is that it allowed for ‘automatic licensing’. This provision allowed a generic manufacturer who has made a ‘significant investment’ and is already producing and marketing a drug in India that will be patent protected from 2005 (e.g. patent applications place in the ‘mailbox’ between 1995 and 2004) to continue to produce the generic version. However, they will need to pay a ‘reasonable royalty’ to the patent holder. Clearly, the interpretation of ‘reasonable’, which was not defined, could lead to quite substantial price increases.
Strategies for ensuring the affordability of drugs within the context of TRIPS compliance could include:
- Specifying what would be a ‘reasonable royalty’ under the ‘automatic licensing’ clause and for ‘compulsory licensing’. For example, the 1970 Indian Patent Act, placed a royalty ceiling at 4% of the value of sales when the equivalent of ‘compulsory licences’ were granted for non-drug products (as drug patents were not covered in the original Act).
- Streamlining the process of granting compulsory licences to ensure that they are issued within the shortest time possible.
- Exploring opportunities for parallel importation.
- Making use of the Bolar exception so that generic drugs can be introduced as soon as a patent expires.
- Applying international price benchmarking regulations on drugs under patent protection. A number of countries undertake pharmacoeconomic evaluations to determine an ‘acceptable price’ for new drugs, taking into account the benefit of the new drug relative to other drugs that exist for treating the same health condition. It may be worthwhile exploring the possibility of benchmarking prices for the new drug against prices charged in such countries (e.g. at the mean price across countries conducting pharmacoeconomic evaluations of new drugs).
- Introducing regulations to limit the extent to which pharmaceutical companies influence medical practitioners’ prescribing practices (e.g. outlawing any ‘incentives’ to practitioners).
THE PERSPECTIVE OF MULTI-NATIONAL DRUG MANUFACTURERS
Some of the issues that may be of assistance in preparing your argument include:
- The pharmaceutical industry is a very important component of the global economy. The global value of the pharmaceutical industry was $566 billion in 2005, which is greater than the Gross National Income of all countries in Sub-Saharan Africa together.
- Multi-national drug manufacturers are the main developers of new drugs, which lengthen life and enhance its quality.
- It costs on average about $800 million to develop and test a new drug before it can be approved for use. Globally, pharmaceutical companies spent $30.4 billion in 2001 on research and development (R&D). Patent protection is required so that companies can recoup the cost of this R&D.
- The effective period of patent protection is far shorter than 20 years, because it takes so long to get approval from drug regulatory authorities to sell the drug. Companies have to apply for such approval/drug registration in each country in which they wish to sell the drug.
THE PERSPECTIVE OF INDIAN GENERIC DRUG MANUFACTURERS
Some of the issues that may be of assistance in preparing your argument include:
- India is the 4th largest producer of pharmaceuticals in the world in terms of volume and ranks 13th in terms of the value of sales of pharmaceutical products.
- Indian pharmaceutical companies have an annual turnover of $5 billion and export drugs to the value of $3.2 million. The consulting firm McKinsey projects that the Indian pharmaceutical industry will grow to $25 billion by 2010.
- India is the world’s leading supplier of generic medicines, with two-thirds of its exports of generic medicines going to developing countries.
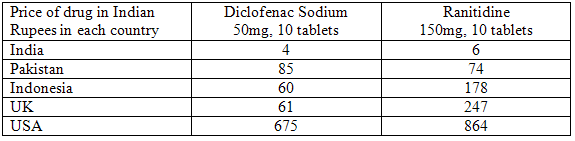
- Indian generic products have contributed to the reduction of price of essential medicines. For example, Indian generic antiretrovirals reduced the price from as much as $10,000-$15,000 per year of treatment to as little as $140 per year for a first-line combination therapy. Other examples of price differences are given in the table below.
- The amendments to the Patent Act will not only prevent Indian generic manufacturers from producing generic versions of new drugs appearing on the market in future, but also from producing generic drugs that have been on the market since 1995 (and where patent applications have been lodged in the ‘mailbox’), including many antiretrovirals.
- Nonetheless, representatives of the industry do not seem perturbed by the new patent regime and the current mood is one of optimism. Representatives argue that only 10 to 12% of the drugs in the market and 5 out of 300 essential drugs qualify for patent protection. Moreover, with a significant number of drugs going off patent over the next four or five years, business prospects for the industry continue to look good, despite the restrictive new Act. According to the Chief Economist of Morgan Stanley, an estimated $40 billion worth of drugs are going off patent. According to estimates by the Organisation of Pharmaceutical Producers of India (OPPI), around $60 billion worth of the generics market will be created in the developed world due to patent expiry.
- Indian industry’s efficient process development and modern manufacturing equipment; highly skilled labour force with excellent chemical synthesis capabilities and cost advantages provide opportunities for business partnerships with foreign manufacturers. Basic production costs in India are up to 50% lower than in the US. Therefore, overseas generic players are eyeing India for setting up low cost manufacturing facilities which will mainly act as sourcing centres for their international operations.
THE PERSPECTIVE OF CIVIL SOCIETY AND HUMAN RIGHTS GROUPS
Some of the issues that may be of assistance in preparing your argument include:
- About half of all patients on ARVs in developing countries use generic drugs produced in India.
- The amendments to the Patent Act will not only prevent Indian generic manufacturers from producing generic versions of new drugs appearing on the market in future, but also from producing generic drugs that have been on the market since 1995 (and where patent applications have been lodged in the ‘mailbox’), including many ARVs.
- In one instance where a multi-national pharmaceutical company was given exclusive marketing rights in India for a drug they had developed, the price of that medicine increased ten-fold.
- The cost of research and development (R&D) to multi-national pharmaceutical companies is estimated to be about 10-16% of the value of their turnover. However, ‘marketing and administration’ costs amount to about 36% of turnover. R&D costs are smaller than the value of profits made by multi-national pharmaceutical companies. For over two decades, the pharmaceutical industry has been the most profitable in the United States. (In 2003, for the first time, the industry lost its first-place position, coming in third, behind "mining, crude oil production," and "commercial banks.").
- In the last quarter of the 20th century, the world’s eleven largest drug companies introduced 1,393 ‘new’ drugs. Only 13 were aimed at tropical diseases and only 4 of these were developed by commercial pharmaceutical companies (the others were developed by public initiatives).
- TRIPS is silent on price control of patented products
- Compulsory Licensing in India is cumbersome and time consuming.
THE PERSPECTIVE OF HOUSEHOLDS
Some of the issues that may be of assistance in preparing your argument include:
- The price of generic drugs for major causes of ill-health can be anything from 10 to 80 times cheaper than brand-name originator products.
- Private health insurance in India has limited coverage. In any event, for those who do have insurance, only inpatient care for non-chronic health conditions qualifies for reimbursement. In such a situation, most households have to cover the costs of health care themselves, and have to do this on an out-of-pocket basis.
- Ill health and resulting medical expenditures are one of three most important reasons why households are falling into poverty in India. Of the expenditure incurred by households on outpatient and inpatient care, a large chunk goes towards the purchase of drugs. Estimates based on the 55th round of the National Sample Survey Organisation’s consumption expenditure survey (in 2005) indicate that drugs account for 83% and 77% of the expenditures incurred on outpatient treatment by rural and urban households respectively. Spending on drugs constitute 56% and 47% of the expenditures incurred on inpatient care by rural and urban households.
- As important as the prices of drugs are, so are the prescribing practices of doctors, which market representatives carefully nurture through periodic visits and attractive rewards. Doctors in turn are dependent on market representatives for updated technical information, as opportunities for continuing medical education are limited. This relationship of mutual dependence between pharmaceutical marketing agents and doctors significantly influences the types of drugs that are prescribed and the resulting costs to the patient.
- Patients have little access to technical information about drugs – especially information about side effects – and are consequently very dependent on the decisions of doctors during their treatment.
- The number of people infected with HIV in India had grown to 4.5 million in late 2002.
