|
1
|
|
|
2
|
|
|
3
|
- OVERVIEW & EPIDEMIOLOGY
- History
- Legal Definitions
- Models of causation
- Risk factors
- CLINICAL & COMPENSATION ASPECTS
- Classification
- Specific clinical conditions
- Compensation
|
|
4
|
- History
- Legal Definitions
- Models of causation
- Risk factors
|
|
5
|
|
|
6
|
|
|
7
|
- Crepitus (crackling sound in subcutaneous tissue)
- Muscle spasm
- Muscle weakness
- Reduction of range movement
- Swelling
- Tender trigger points in muscles
- Tenderness
|
|
8
|
- STAGE 1
- Pain, aching & tiredness of limb during work
- Improve overnight
- Most often reversible with rest alone
- Sometimes guided exercise and treatment is required
|
|
9
|
- STAGE 2
- Recurrent pain, aching and tiredness earlier in day
- Persist at night and may disturb sleep
- Physical signs (e.g. swelling) may be visible
|
|
10
|
- STAGE 3
- Persistent pain, aching, weakness and fatigue even if not been working
for some time
- Sleep is often disturbed
- This can be irreversible if it is not treated appropriately
|
|
11
|
- De Quervain’s syndrome and Carpal Tunnel Syndromes were diagnosed during
the past 2 years
- She received steroid injections into the relevant tendon sheaths
- Twice surgery
- Only little improvement
- And now it is “all in the mind”…
|
|
12
|
- R40,000 later (pain & suffering & loss of income excluded)
- Nobody ever asked her “WHAT ARE YOU DOING AT WORK?” …
- !!!@#$%^&*()!@#$%^&&?!!!
- Typical doctor / specialist …???!!!
|
|
13
|
- Results from a number of factors
- where the work environment and the performance of the work contribute
significantly, but in varying magnitude, to the causation of the
disease.
- Some of the disorders have well defined signs and symptoms
- E.g. rotator cuff tendinitis, carpal tunnel syndrome and acute
prolapsed inter-vertebral disc.
|
|
14
|
- Many others are less well defined:
- E.g. myalgic conditions involving pain, discomfort, numbness and
tingling sensations throughout the neck shoulders, upper limbs and
lower back.
- These types of disorder, that are sometimes called non-specific WMSDs,
often cannot be diagnosed with respect to a clinical pathology but they
may still result in physical impairment and disability.
|
|
15
|
- WMSDs therefore, cover a wide range of inflammatory and degenerative
diseases of the locomotor system. They include:
- Inflammations / degenerations of tendons (tendinosis, tendinitis and
tenosynovitis), especially in the forearm-wrist, elbow and shoulder,
evident in occupations involving prolonged periods of repetitive and
static work;
- myalgias, i.e. pain and functional impairments of muscles, occurring
predominantly in the shoulder-neck region, that occur in occupations
with large static-work demands;
|
|
16
|
- compression of nerves – entrapment syndromes – occurring especially in
the wrist and forearm;
- degenerative disorders occurring in the spine, usually in the neck or
lower back, especially in those performing manual handling or heavy
physical work. However, they may also occur in the hip or knee joints.
- These disorders are chronic, and symptoms usually occur only after
exposure to work-related risk factors for a period of time.
|
|
17
|
- 2.3. Occupational musculo-skeletal disorders
- 2.3.1 Musculo-skeletal diseases caused by specific work activities or
work environment where particular risk factors are present. Examples of
such activities or environment include:
- (a) rapid or repetitive motion
- (b) forceful exertion
- (c) excessive mechanical force concentration
- (d) awkward or non-neutral postures
- (e) vibration
|
|
18
|
- WRULDs is a collective term for a group of occupational diseases that
consist of musculo-skeletal disorders caused by exposure in the
workplace affecting tissues (muscles, tendons, nerves, blood vessels,
joints and bursas) of the hand, wrist, arm and shoulder.
|
|
19
|
- Repetitive Strain Injury (RSI) – Australia
- Cumulative Trauma Disorder (CTD) – USA
- Occupational Cervicobrachial Disorder – Japan & Sweden
- Work-related upper limb disorder (WRULD) – E.U.
|
|
20
|
- Not a new problem
- 1713: Ramazzini – serious disease caused violent and irregular motions
and unnatural postures of the body".
- Scrivener's Palsy – incessant driving of pewn over paper causes intense
fatigue of hand & arm because of continuous strain of the muscles
& tendons
|
|
21
|
- 1830s: Sir Charles Bell
- writer’s cramp in male clerks in British Civil Service
- steel nibs vs goose-quill pens
- Late 19th Century:
- musicians, telegraphists, cowherds, hammersmiths, seamstresses,
bricklayers, etc.
|
|
22
|
- Telegraphist’s cramp
- Hop picker’s gout
- Fisherwoman’s finger
- Upholsterer’s hand
- Gamekeeper’s thumb
- Cotton-twister’s hand
- Tennis elbow
- Pizza-cutter’s wrist
- Nintendonitis (Nintendo® play station – ‘computer game wrist’
in children)
|
|
23
|
- Keypunch operators 16-28%
- Typists 13%
- Cash register operators 11-16%
- Packing machine operators 12%
- Assembly line workers 16%
|
|
24
|
- Work maximum of 5 hours/day
- Take 10 minutes rest / hour
- Do less than 40,000 keystrokes / day
- Job Rotation
|
|
25
|
- Data processors g all
screen-based operators
- 1978/9 = 762 cases
- 1981/2 = 2263 cases (h 297%)
|
|
26
|
- 90,000 employees
- Cost
- $15,5 million
- $1,8 million medical cost
- (excluding common law claims)
|
|
27
|
- Collective term - range of conditions characterised by discomfort or
persistent pain in muscles, tendons and other soft tissues, with or
without physical manifestations
- Usually caused or aggravated by work, thought to be associated with repetitive
movements, sustained or constrained postures and/or forceful movements
- Psychosocial factors, including stress in the working environment, may
be important in the development of RSI
- National Occupational Health & Safety Commission (1986)
|
|
28
|
- Young (±40 years)
- Women with children at home
- Stomach-related stress conditions
- Smokers
- Progressive glasses and/or bifocals
- Did not exercise
- Poor social conditions
- Monotonous work
- Lack of job control
- Recent increase in workload
|
|
29
|
- A psychosomatic symptom complex
(epidemic of mass hysteria)
- Socio-political phenomenon
vs.
medical condition
|
|
30
|
- Cooper vs. Commonwealth (1987)
- Employer not guilty of negligence
- Plaintiff had no injury
- Awarded all costs against the plaintiff
|
|
31
|
- RSI = an occupational neurosis
- Not associated with localised pathology
- Reversible with normal use
- No residual, permanent disability
|
|
32
|
- Editorial decision to publish articles that emphasised the non-physical
nature of RSI
|
|
33
|
- Vague definition
- Epidemic spread
- Treatment unsuccessful
- Self-employed unaffected
- Repetitive, monotonous tasks
- Low job satisfaction
|
|
34
|
- Regional Pain Syndrome
- Work-related and non-occupational risk factors
- E.g. carpal tunnel syndrome
|
|
35
|
|
|
36
|
- WRULDs cost
- Nordic Countries –0,5% GNP
- Netherlands – 2% GNP
- UK £1.25 billion per year
- Sources:
- HSE (1996)
- EU Agency for Safety & Health at work (1990)
|
|
37
|
- Limited data – need research
- WRULDs expected to be higher than industrially developed countries – h excessive physical
demands made on workers
- SAMOSA (SA Musculoskeletal
Surveillance Action
Group)
|
|
38
|
|
|
39
|
- 1. Biomechanical
- Excessive loads, force, repetition
- Abnormal postures
- Compression. Ischaemia. Microtears. Muscle fatigue.
Metabolic changes. Inflammation.
- 2. Psychosocial
- Somatising disorders (e.g. work stress, depression)
- Industrial relations conflict
- changing nature of work
- medicalised via workers' compensation
|
|
40
|
- 3. latropenic-(Hadler)
- High background rate of aches and pains
- Misattribution to work as primary cause
- 4. Technological
- Automation, specialisation, electronic data processing
|
|
41
|
- WRULDs are caused, aggravated or precipitated by one or more of the
following risk factors, singly or in combination:
- Task-related factors
- highly repetitive upper limb movements
- awkward and/or static working postures
- Movements at the extremes of reach
- Contact stress (e.g. uncomfortable gripping and twisting, sharp edges
to hand tools, desk edges, etc.)
- high force requirements
- duration of exposure to tasks
|
|
42
|
- Environmental-related factors
- Vibration
- Low temperatures (Cold)
- Lighting
- Work organisation (e.g. rotation, hours, shifts, high task pressure,
conveyor belt))
|
|
43
|
- Job dissatisfaction: +
- Monotonous work: ++
- Perceived intensified work load: ++
- Lack of job control: ++
- Lack of job clarity: ++
- Job stress leading to excessive pressure such as high job demands, time
pressures and lack of control;
|
|
44
|
- Depression / burn out / affirmative action
- Lack of social support from supervisors or co-workers;
- tasks requiring high levels of attention and concentration are related
to increased muscle tension, changing thresholds for the perception of
pain and fatigue.
- “compensitis”
|
|
45
|
- Individual differences
- All individuals are different and for biological reasons there may be
some people who are more or less likely to develop an WRULDS.
- Individual differences may also have implications for employees
reporting WRULDS type conditions.
- Genetic predisposition
- new employees - time to acquire the necessary work skills and/or rate of
work;
- difference in competence and skills;
|
|
46
|
- Anthropometry - workers of varying body sizes, ie height, reach etc.;
- vulnerable groups, eg older, younger workers and new or expectant
mothers;
- Gender
- health status and disability;
- individual attitudes or characteristics that may affect compliance with
safe working practices or reporting of symptoms .
- Smoking: Some association with LBP
|
|
47
|
- Heavy manual labour
- Lifting, twisting, awkward motions
- Sitting
- Driving, whole body vibration
- Shorter duration of employment
- ? Psychosocial: monotonous work, low motivation, lower rating by
supervisor
|
|
48
|
- Smoking
- Taller
- More births
- Heavy alcohol
|
|
49
|
|
|
50
|
|
|
51
|
|
|
52
|
|
|
53
|
|
|
54
|
|
|
55
|
|
|
56
|
- Classification
- Specific clinical conditions
- Compensation
|
|
57
|
- TYPE 1
- Well-defined musculo-skeletal conditions & nerve entrapment
syndromes affecting the upper limbs
- Carpal Tunnel Syndrome, De Quervain’s
- Relatively clear cut characteristics & established treatment methods
|
|
58
|
- TYPE 2
- Regional Pain Syndrome
- Widespread dissemination of symptoms between neck & hand
- Regional allodynia & hyperalgesia g neural sensitisation & pain
|
|
59
|
- Tendon-related disorders
- Nerve-related disorders
- Bursa-related disorders
- Blood vessel disorders
- Other
|
|
60
|
- Tendonitis
- Confusion with terminology
- Rare condition
- Inflammation of tendon & tendon muscle
- (e.g. Achilles tendon in conjunction with tendinosis)
- Promote collagen production & reduce paratendon inflammation
|
|
61
|
- Tendinosis - common
- Sports Medicine
- Intratendinous collagen degeneration due to
- Aging
- Microtrauma (chronic overuse repetitive movements)
- Vascular compromise
- Examples:
- epicondylitis, rotator cuff
syndrome
|
|
62
|
- Treatment of tendinosis
- Combat collagen breakdown
- Relative rest for reasonable period
- Strengthening and graduated loading of tendon (eccentric)
- Facilitate collagen production & maturation gnormal strength
|
|
63
|
- Tenosynovitis
- Rapid repetitive movements especially of hands and fingers g
- Inflammation of synovial lining of the tendon
sheath g
- swelling g pain g
- restricted movement of tendon in sheath
- Repeated exposure g hscar tissue g h pain g imobility g istrength
- Examples:
- Trigger Finger, De Quervain’s
|
|
64
|
- Nerves need to undergo mechanical changes (compression, elongation,
cross-sectional changes, etc.) for normal functioning
- â mechanical changes g physiological changes (âaxoplasmic flow, etc.)
|
|
65
|
- Dysfunctional nerve g
- Pain
- Paraesthesia
- Sensory changes
- in areas supplied by nerve
|
|
66
|
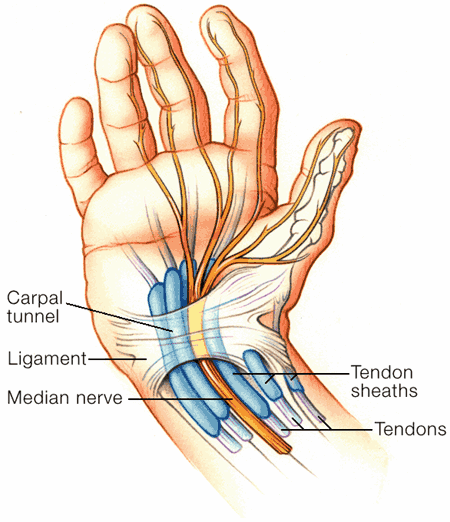
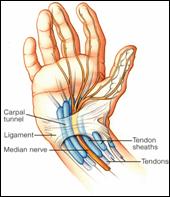
- Carpal Tunnel Syndrome
- Pronator Teres Syndrome
- Cubital Tunnel Syndrome
- Guyon tunnel Syndrome
- Radial Tunnel Syndrome
- Anterior Interosseous Nerve Syndrome
- Posterior Interosseous Nerve Entrapment, etc.
|
|
67
|
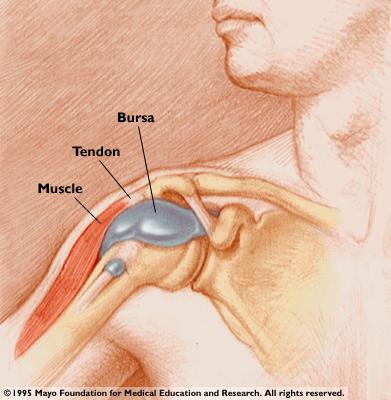
- Fluid-filled sacks that protect muscles, tendons & skin from
friction against bones during joint movement
- Overexertion g
inflammation (bursitis) g swelling & dull, aching pain
- Examples:
- Olecranon bursitis (beat elbow)
- Subacromial burisits
- Subdeltoid bursitis
|
|
68
|
- Usually due to vibration or hammering g vasospasm & i circulation
- Excessive exposure g i circulation +
neurological findings (i motor function of hand and arm)
- Examples:
- Raynaud’s Phenomenon
- Hand Arm Vibration Syndrome
- Hypothenar Hammer Syndrome
|
|
69
|
- Effect on muscles and joints
- Problematic to prove objectively
- Controversial
- Static loading
- Occurs proximally when repetitive movement occurs distally
- Static loading g
muscle imbalances & trigger points g pain
- Examples:
- Tension neck syndrome, myalgia, strains, etc.
|
|
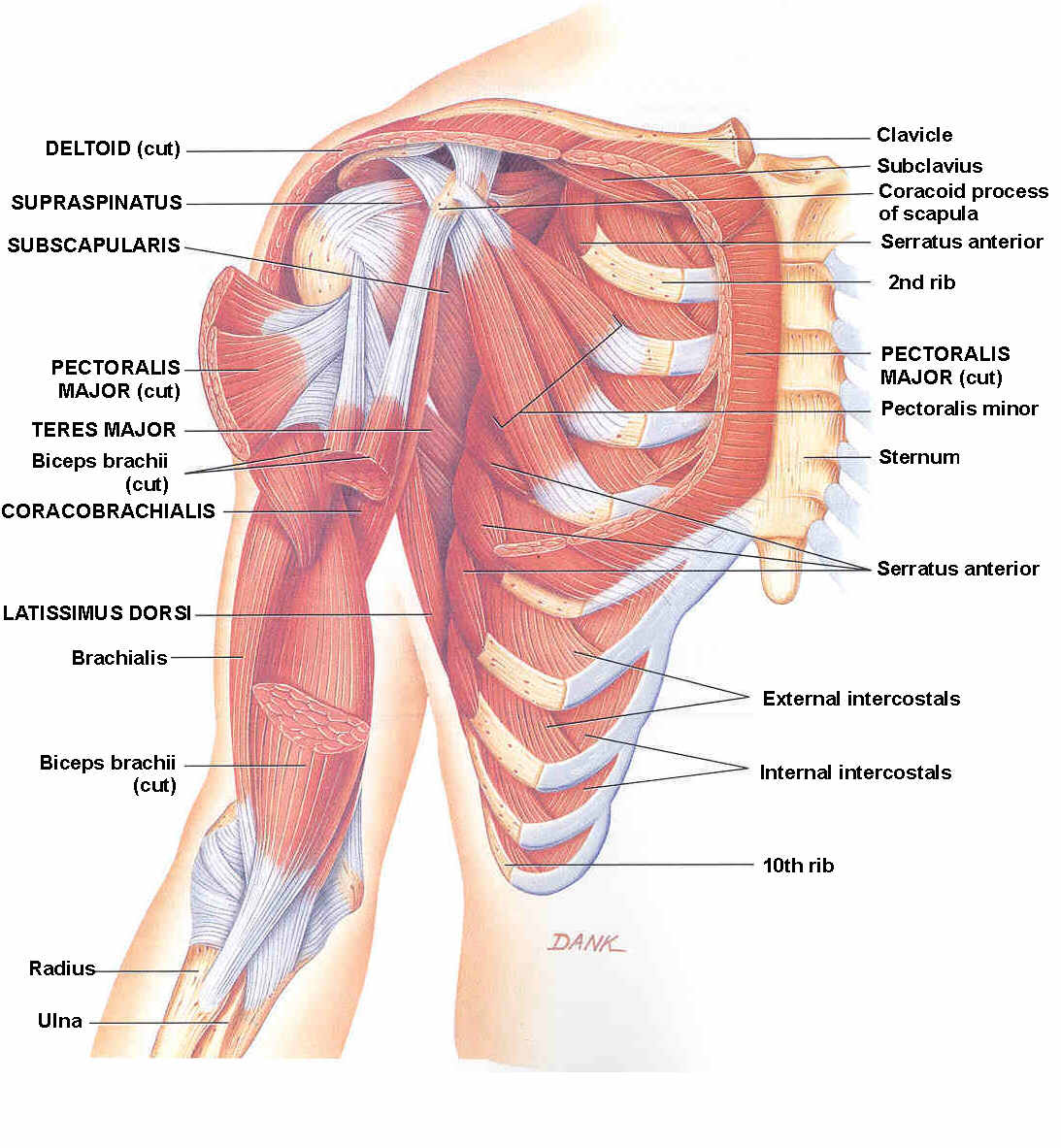
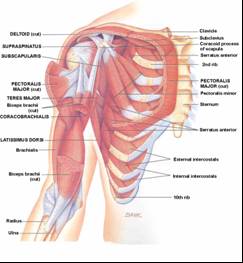
70
|
- Bicipital tendinosis
- Infraspinatus tendinosis
- Partial tear of the rotator cuff
- Subacromial bursitis
- Subdeltoid bursitis
- Subscapularis tendinosis
- Supraspinatus tendinosis
- Tendinosis of the shoulder
|
|
71
|
- Executing repetitive overhead movements, static loading and/or sustained
postures.
- Prone to develop bursal side tears secondary to impingement
- Sign of rotator cuff lesions = pain exacerbated by abduction against
resistance.
|
|
72
|
- Limited by pain towards the end of the active range of movement
- Passive range of motion ± normal
- Acute rotator cuff tendinosis ≤12 weeks duration.
- Chronic rotator cuff rupture = marked difficulty initiating abduction
with weakness and limitation of movement
- “painful arc” - 70o to
120o abduction
|
|
73
|
- Belt conveyor assembly
- Carrying load on shoulders
- Construction work
- Electrical work
- Lifting
- Overhead assembly
- Overhead painting
- Overhead welding
- Packing
- Punch press operation
- Reaching
- Work with the arms away from the body
|
|
74
|
- Rupture of the long head of the biceps
- Pectoralis major strains
- Levator scapulae syndrome
- Fractures around the shoulder joint.
|
|
75
|
- “Tennis Elbow” -
Pain at epicondyle
|
|
76
|
- Often starts as an acute direct injury to the site of the muscle origin
which progresses to an epicondylitis
- Work action:
- Unusual forces (power grasp),
- Repetition
- Forceful gripping
- Repeated supination and pronation.
|
|
77
|
- Overuse of
- finger flexors
- wrist flexors / pronators
|
|
78
|
- Resting forearm near elbow on a hard surface
- Resting forearm near elbow on sharp edge
- Resting forearm near elbow while reaching over obstruction
- Repetitive or static elbow flexion
|
|
79
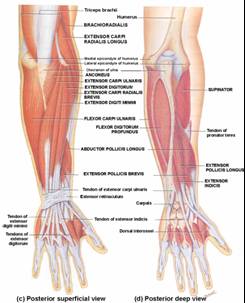
|
- Stenosing tenosynovitis of the abductor pollices longus and extensor
pollices brevis tendons
- Tendons of the forearm are stretched and rub against the radial styloid g inflammation of tendon
sheath
|
|
80
|
- Presents with pain & localised swelling over styloid process of
radius
- Common variant : localised swelling at base of the thumb &
thickening of fibrous sheath (extensor retinaculum).
|
|
81
|
- De Quervain’s can results from overuse of the thumb
- such as in the repetitive grasping of a straight handled tool
- (e.g. screwdriver, endo files of dentist).
|
|
82
|
- Diagnostic criteria
- Pain and tenderness localised to the radial aspect of the wrist
- PLUS positive Finkelsteins's test
- Sometimes a palpable nodule in course of
Abd. pollicis longus & Ext. pollicis brevis.
|
|
83
|
- Differential Diagnoses
- Degenerative arthritis of trapeziometacarpal joint
- Grind Test
- Painful in degenerative arthritis
- No, little pain in De Quervain's
|
|
84
|
- Differential Diagnoses
- Degenerative arthritis of trapeziometacarpal joint
- Post-partum women
- Intersection Syndrome
- Wartenberg's Syndrome
- Radial sensory nerve entrapment causing significant pain in the lower
third of the forearm
|
|
85
|
- Stenosing tenosynovitis and/or tendinosis of flexor tendons
- Inability to move fingers or thumb smoothly
- Locking of affected digit, with or without pain.
|
|
86
|
- Hand tools that have sharp edges pressing into the tissue
- Hand tools whose handles are too far apart for user.
- Repetitive movements with repeated or prolonged gripping or pinching can
also cause operating trigger finger.
- Investigate concomitant diseases
and/or other reasons for trigger finger
- rheumatoid arthritis
- diabetes, etc.
|
|
87
|
- Condition which results from direct or indirect pressure on nerves
- Common ailment affecting the wrist and hand
- Majority of cases not caused by work
|
|
88
|
- Specific occupations where wrists are in abnormal positions for
prolonged periods with highly repetitive movements
- Tenosynovitis of flexor tendons
- Pressure on the median nerve in the carpal tunnel
- Buffing
- Grinding
- Prehensile task especially in extremes of flexion, extension and ulnar
deviation
- Assembly work
- Typing
- Packing
- Scrubbing
- Hammering
- Repetitive or forceful grip
- VDT work
- Polishing
- Sanding
|
|
89
|
- SYMPTOMS
- Symptoms start with a gradual onset of
- tingling and numbness in the fingers
- Can progress to
- pain
- Clumsiness
- muscle atrophy in the hand.
|
|
90
|
- CLINICAL DIAGNOSIS
- Positive Tinel’s Sign
- pain, numbness, or tingling in the median nerve distribution resulting
from tapping over the proximal wrist crease
- PLUS
- Positive Phalen’s sign or reverse Phalen’s sign
- pain, numbness, or tingling in the median nerve distribution resulting
from complete palmar flexion and dorsiflexion respectively, of the
wrist for 60 seconds
|
|
91
|
- CARPAL TUNNEL AS INJURY
- Direct injury to the wrist area
- Acutely
- haematoma g pressure
on the nerve
- More sub acutely
- like a fracture g swelling
/ deformity.
|
|
92
|
- Punch press operation
- Assembly work
- Wiring
- Packaging
- Use of pliers
- Buffing
- Grinding
- Polishing
- Sanding
- Punch press operation
- Sawing
- Cutting
- Use of pliers
- “Turning” controls such as on motorcycle
- Inserting screws in holes
- Forceful hand wringing
|
|
93
|
- Radial Tunnel Syndrome
- Guyon (Ulnar) Tunnel Syndrome
- Pronator Teres Syndrome
- Anterior & posterior Interosseous Syndrome
- Intersection Syndrome.
|
|
94
|
- Medical assessment
- Medical history
- The employee’s current medical history:
- site and distribution of the symptoms
- quality (type, character)
- severity (intensity, frequency, duration)
- progression of the symptoms.
- Physical examination
- Special investigations
|
|
95
|
- Functional capacity evaluation
- E.g. the employee is able to type, but develops symptoms after
continuous typing for 30 minutes.)
- This might be simple and straightforward …
- in complicated cases a formal occupational therapy and / or
physiotherapy assessment
- Job analysis / Ergonomic assessment
- Assess the employee’s working environment(s) for human and
environmental risk factors.
|
|
96
|
|
|
97
|
- Burning sensation
- Fatiguability
- Loss of grip strength
- Loss of normal sensation
- Muscle spasm
- Muscle weakness
- Pain
- Paraesthesia (tingling)
- Sensation of cold
- Swelling
|
|
98
|
- Crepitus (crackling sound in subcutaneous tissue)
- Muscle spasm
- Muscle weakness
- Reduction of range movement
- Swelling
- Tender trigger points in muscles
- Tenderness
|
|
99
|
- Symptoms may not always be accompanied by objective signs
- Any one symptom or sign is not indicative of WRULDs and some may be
common with normal function
- Very few sufferers experience all the symptoms
- The symptoms do not appear in any particular order
|
|
100
|
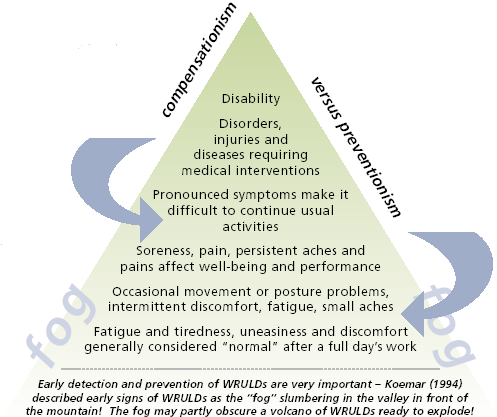
- STAGE 1
- Pain, aching & tiredness of limb during work
- Improve overnight
- Most often reversible with rest alone
- Sometimes guided exercise and treatment is required
|
|
101
|
- STAGE 2
- Recurrent pain, aching and tiredness earlier in day
- Persist at night and may disturb sleep
- Physical signs (e.g. swelling) may be visible
- Refer for physiotherapy and ergonomic assessment to prevent recurrence
|
|
102
|
- STAGE 3
- Persistent pain, aching, weakness and fatigue even if not been working
for some time
- Sleep is often disturbed
- This can be irreversible if it is not treated appropriately
|
|
103
|
- Require summary of
- work environment
- work process
- work actions
- If necessary, photos, diagrams and/or extra reports to explain the
employee’s work actions may be very helpful
|
|
104
|
- RISK FACTORS
- Repetitive actions with short cycles
- Forceful movements
- Static loading of muscles
- Any postures held for a long time, especially awkward postures.
- Forceful gripping and twisting
- Poor work organisation – low level of control over work rate and no
breaks
|
|
105
|
- RISK FACTORS
- Psychosocial stress at work and fatigue
- Cold environment or handling chilled or frozen products
- Vibration
- Overhead working postures or jobs with minimal movement and non-optimal
sustained postures.
- High-risk jobs - Combination of repetitive, forceful movements, awkward
postures, static loading
|
|
106
|
- Perform special investigations
- if it is essential for the accurate diagnosis and treatment of the
disorder
- to investigate and eliminate other causes
- Examples
- X-rays
- strength testing
- range of motion testing
- electromyography (EMG) analysis
- isokinetic dynamometry
- Get prior authorisation for MRI
scans
|
|
107
|
- OHP: explain pathology of tendinosis
- Most vulnerable employees
- Those with symptoms of short duration and still able to work
- Should they continue without Rx g exacerbate condition
|
|
108
|
- Cryotherapy (ice)
- Electrotherapeutic modalities (Physiotherapy)
- Non-steroid anti-inflammatory drugs (e.g. Voltaren)
- Infiltration with corticosteroids
- Inhibits collagen repair g avoid
|
|
109
|
- Initial treatment may include rest
- Compression and elevation
- Temporary job change
|
|
110
|
- Biomechanical deloading
- Collagen degeneration & mechanical overload g tendinosis
- Mechanical overload due to
- Work environment
- Work tasks (repetition, force, posture, vibration, etc.)
- Individual biomechanics (trigger points, muscle imbalances)
- Correct biomechanics
- Movement patterns
- muscle imbalances
- Equipment used / environment
|
|
111
|
- Immobilise – Splintage (occupational therapy)
- Load-decreasing devices
- imechanical load on
collagen
- Examples
- Tenosynovitis of forearm, wrist, fingers, etc.
|
|
112
|
- Mobilise – manual therapy (physiotherapy)
- Mobilise – exercise therapy to appropriately strengthen the tendons and
muscles.
- Graded loading of tendon g improved collagen alignment & cross linkage g improved strength
- Eccentric training drills g stimulate mechanoreceptors in tenocytes g hcollagen production
- Collagen production key to tendinosis recovery
- Re-introduction to the workplace (Work hardening and ergonomics
adjustments)
|
|
113
|
- Pscychological evaluation
- Surgery
- where indicated as last resort
|
|
114
|
- Interaction with the therapist
- OMP, OHN, employee, employer, physiotherapist, occupational therapist,
biokinethesist, ergonomist, medical specialist g
- Similar understanding of tendinosis pathology
- Coordinated approach
- Realistic time frame for rehab
(months, not weeks)
- Short duration symptoms ~ resolve fully in 2-3 months
- Chronic symptoms ~ 4-6 months
|
|
115
|
- For the OHN as primary contact
- For the OMP to work up the case
- Reporting to the Compensation Commissioner (OMP)
- Reporting to Dept Labour / DME (Employer)
|
|
116
|
- A reportable occupational disease to the
- Compensation Commissioner
- Inspectorate of the nearest Dept of
- Labour
- Minerals and Energy
- An occupational medicine practitioner should preferably do the
notification.
|
|
117
|
- Occupational Disease = WRULD caused by repetitive movements (¹ injury )
- Occupational Injury = Complication of initial occupational injury
- Example: Fracture of the forearm Ú
- Tenosynovitis (because no work hardening)
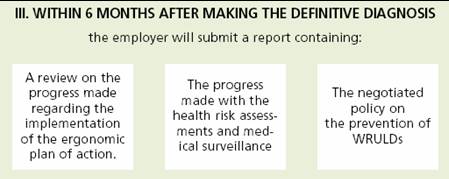
- Here WRULD should be reported to Compensation Commissioner on the
Progress Medical Reports i.t.o. occupational injury.
|
|
118
|
- Report to the Compensation Commissioner so that payment of medical
costs, sick leave and compensation could be considered in terms of the
COID Act.
- Prevention: Report to Provincial Executive Manager of Labour / Regional
Principal Inspector of Mines
|
|
119
|
- W. Cl. 1
- Employer’s Report of an Occupational Disease
- W. Cl. 14
- Notice of an Occupational Disease and Claim for Compensation
- W. Cl. 110
|
|
120
|
- W. Cl. 301
- First Medical Report in respect of a Work-Related Upper Limb Disorder
(WRULD)
- W. Cl. 301 must be used instead of the usual W. Cl. 22
- All other reports that may be relevant
|
|
121
|
- W. Cl. 6
- Monthly Resumption Report
- W. Cl. 302
- Progress/Final Medical Report in respect of a Work-Related Upper Limb
Disorder (WRULD)
- Progress medical reports - monthly
- W. Cl. 302 must be used instead of the usual W. Cl. 26
|
|
122
|
- Description of residual impairment by the treating doctor (W. Cl. 302)
- Most employees will recover and return to work
- only a small percentage will suffer any permanent residual impairment.
|
|
123
|
- Medical treatment
- Vocational rehabilitation, which includes
- Optimising the person’s functional ability through rehabilitation that includes
work hardening, work conditioning, etc.
|
|
124
|
- Addressing problem areas identified in the job analysis / ergonomic
assessment by allowing alterations in the way in which work is
performed through reasonable accommodation:
- workplace environment adaptation
- tool and equipment adaptation
- workstation redesign
- job task modification
- retraining and reassignment
- work schedule modifications
|
|
125
|
|
|
126
|
|
|
127
|
|
|
128
|
|

 Notes
Notes{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}