Content begins here
Main page content
Click to collapse

 LEARNING OBJECTIVES
LEARNING OBJECTIVES
By the end of this module the learner should be able to:
- Recognize the signs of glue ear and cholesteatoma
- Guide patients with glue ear and refer if required
- Guide people on the importance of addressing cholesteatoma as early as possible
- Understand what is Bell’s palsy and how to guide patients
TERMINOLOGY
–– Bell´s palsy
–– Cholesteatoma
–– Complaints associated with cholesteatoma
–– Glue ear Sunken eardrum
–– Polyp
–– Pus
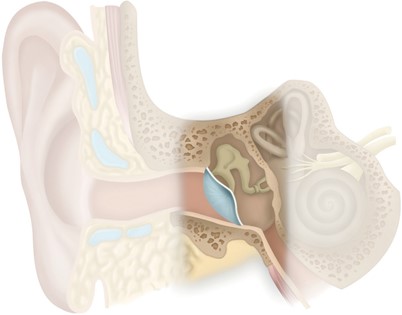
There are a variety of problems, other than infection, that can arise in the middle ear. These issues are explained in detail in this module.
There can be other problems in the middle ear:
- Fluid in the middle ear, called glue ear
- Skin of the ear drum growing in, called cholesteatoma
- Weakness of the facial nerve called Bell’s Palsy
5.1 FLUID IN THE MIDDLE EAR (GLUE EAR)
Who gets glue ear?
 This is most common in young children and can sometimes occur in adults.
This is most common in young children and can sometimes occur in adults.
What happens?
Glue ear is when there is fluid behind an intact eardrum. It is different from an ear infection (acute otitis media) because there is acute pain in the ear or high temperature.
It can cause hearing impairment, because the fluid stops movement of the bones of hearing. In children this can lead to speech problems.
What are the complaints?
- Fullness of ear or dull ache
- Difficulty in hearing
- Speech problems e.g., child not speaking clearly or delayed speech development
- Child not performing well at school
- There is NO complaint of ear discharge in a glue ear
What will you see?
Use an otoscope to look at the eardrum
- The eardrum will not look normal – it could be dull, it could be sunken but it does NOT have a hole in it.
 At times, you may be able to see some fluid through the eardrum
At times, you may be able to see some fluid through the eardrum- Check both ears
- Test the hearing – There may be slight/moderate hearing impairment
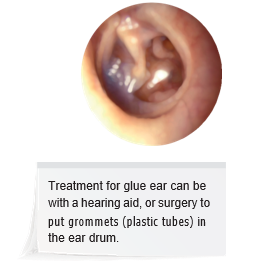
What should you do?
Glue ear usually gets better by itself. It doesn’t always need treatment.
- Reassure the patient and call for review after three months.
REFER IF:
- There is a complaint of speech problems or poor academic performance.
- Hearing impairment persists even after one month.
- Glue ear is only one ear in an adult
- The ear is painful
Refer to an ENT doctor if possible. Where this is not possible, send the patient to a general practitioner.
If a patient with a pulled in ear drum gets repeated infections, or has a hearing loss, refer them to an ENT surgeon
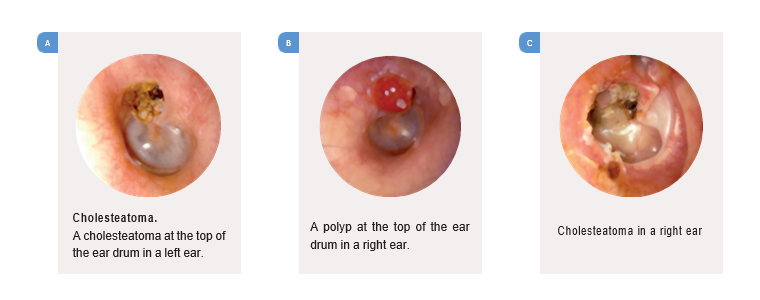
5.2 CHOLESTEATOMA
What happens?
We are not sure what causes cholesteatoma. It can happen in children and adults of any age.
|
What are the complaints?
|
What will you see?
|
 WHAT SHOULD YOU DO?
WHAT SHOULD YOU DO?
- If you suspect cholesteatoma, Refer the patient to an ENT specialist immediately. The only treatment for cholesteatoma is surgery.
- Stress to the patient that untreated cholesteatoma can lead to serious complications and they should get immediate attention.
5.3 BELL'S PALSY
What happens?
At times people may suddenly develop weakness of the face on one side (a disorder called Bell’s palsy). We don’t know what causes this problem and it usually recovers in a few weeks.
What are the complaints?
Inability to close the eye on one side
Watering from that eye
Difficulty in smiling, speaking and sipping drinks
Liquids may leak out of the mouth on affected side
What will you see?
Patient will be unable to close the eye on the affected side.
On smiling, lips don’t move on the affected side
If you ask patient to blow his cheeks, the affected side will not inflate
What should you do?
You should REFER all patients with facial weakness to see a doctor.
If the patient has no earlier history of ear disease, you can reassure them that it will probably resolve in a few weeks time, but still encourage them to see a doctor.
5.4 VIDEOS
![]() Revision - pathophysiology chronic suppurative otitis media
Revision - pathophysiology chronic suppurative otitis media
![]() Revision - suppurative otitis media - consequences and complications
Revision - suppurative otitis media - consequences and complications
![]() Anatomy of the facial nerve as it runs through the temporal bone
Anatomy of the facial nerve as it runs through the temporal bone
![]() Common lower motor neuron facial nerve disorders
Common lower motor neuron facial nerve disorders