 |
| Block 1: Epidemiology |
| EPI12-3: CRITICAL APPRAISAL |
|
| Block 1: Epidemiology |
| EPI12-3: CRITICAL APPRAISAL |
Having read the article and evaluated it in terms of the checklist, we can identify some problems. These are displayed in red.
Title - appropriate
This is not particularly clear. It suggests a simple description of surveillance over 10 years but in fact is mainly about showing the validity of ZPP vs Blood lead monitoring.
Abstract/summary - adequate and not misleading
Literature review - adequacy, appropriate and relevant research problem.
The literature review and introduction seem to be mixed with the methods. Although the US and UK action levels for BPb are given, none is given for South Africa.
The reference to Dornan is for the UK and not SA as the paragraph would lead one to believe. It is difficult to work out what refers to UK and what to SA.
There is a long section on mining and extraction methods which is not relevant.
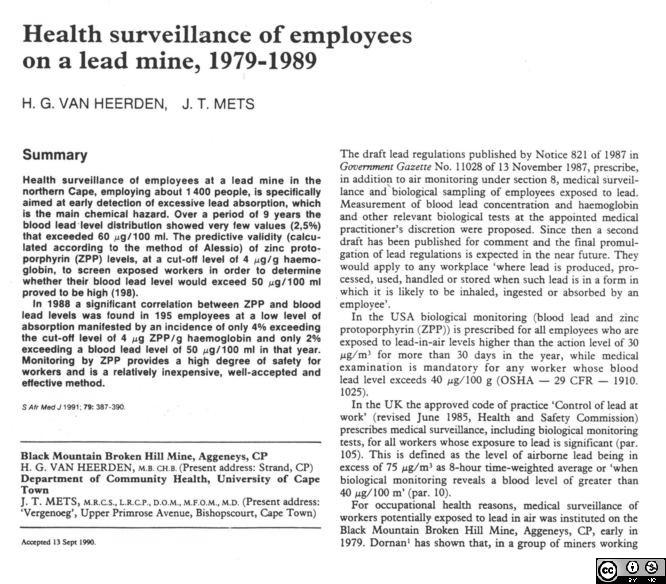
The monitoring programme is poorly described as is the sampling of blood leads. It is not clear how may samples were take over which period. The period in question also seems to begin in 1981 which is different to what is stated in the title. The surveillance programme changed substantially in 1983.
It is unclear why the action level is 60 when 40 is used by the US and the UK and also the WHO health based limit for lead is 40.
Motivation
Aim - Concisely stated. Not stated.
Objectives - attainable and precisely defined, do they relate to aim? Not stated.

Methods: There does not appear to be a methods section per se.
We are also suddenly informed at the end of the medical monitoring section that from 1983 only high risk (and presumably high exposure) workers were followed.
Results
An irrelevant anecdote about an individual worker opens the results section. Only at this point is the WHO health based limit introduced although it is not called this but rather a "recommended level". The ZPP meter was only introduced in 1988 the last year of the period under study! Findings from other studies are quoted as "statements". These have low correlation coefficients (0.7) and only explain half of the variation of blood lead. Although the measure of validity sounds high the specificity is low at 79% leaving room for lots of false negatives which is a concern in a screening programme.
Extraneous results from a group of workers in the lead industry are introduced here with no prior information in the methods, or aims and objectives. The correlation coefficient is similar to 0.7.
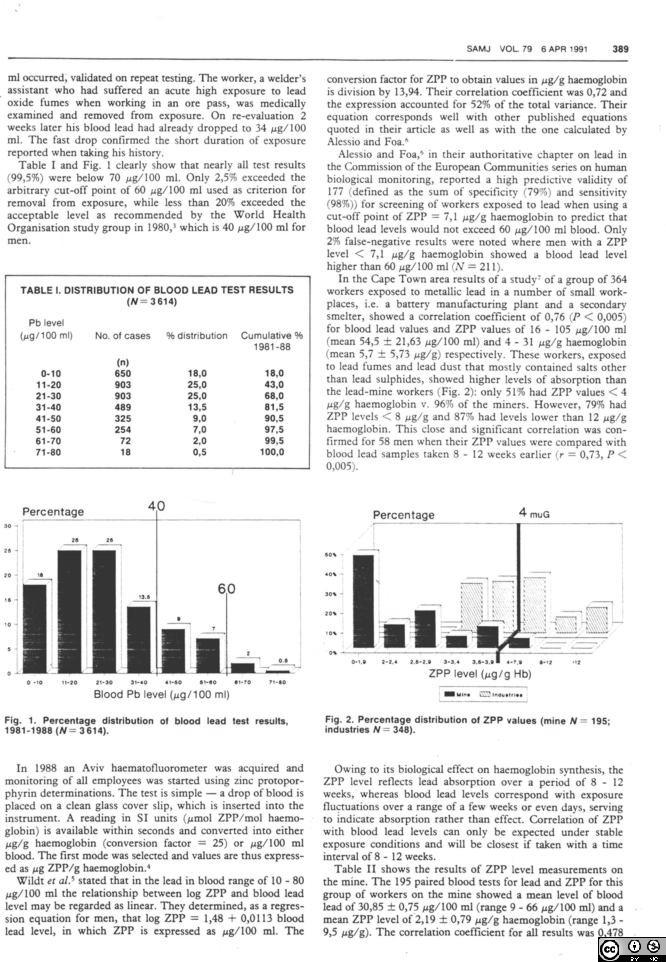
All of a sudden 195 paired samples (blood Pb and ZPP) are introduced without any prior explanation. How were these chosen? The correlation coefficient is much lower at 0.48, but reaches 0.7 for those whose blood lead levels are > 40. It is unclear whether these 195 have been selected as a low exposure group or not. It is known from later studies that the correlation levels are poorer when the exposures are lower. This reduces the preventive value of the ZPP in detecting blood levels that are rising dangerously from lower levels than 40.
Sometimes the cutoff for blood lead is 60 and at other times 50. It is not clear why these are used interchangably.
At no point does their medical examination seem to include neurobehavioural tests which typically pick up abnormalities at levels higher than 40.

Discussion
The very low positive predictive value (this is only called the "predictive value" withouth specifying which one it is, means that only 2% of those who test positive will be truly abnormally high in terms of blood lead. This means it is a poor screening test for this particular population which has a low prevalence of those with blood lead levels higher than 60 - which can be seen from the range which goes from 9 to 66. This once again confirms that a group has been taken which has typically low exposure. Despite the seemingly high values for sensitivity and specificity (not so high) the test is not too useful as a screen as one would find only 2 of every hundred who screen positive to really have high blood leads!
The conclusion states that there is a low risk of excessively absorbing lead even for the WHO criteria. This is simply not true as we are not told what the figure is except in table I where it is quite high at 20% or 1 in 5 workers.
Basically this study is so poorly described in terms of aims, objectives and methods that any results - if one can be clear about what is being described - are pretty much useless and unamenable to interpretation.
![]()
![]()
